
Note: This draft policy has been written for SEN with particular regard to Sp.L.D. It could be expanded to include all SEN, e.g. Moderate Learning Difficulties (low intelligence) etc
The aims of this Policy are to provide an EU SEN Policy, including Sp.L.D.
The objectives of this Policy are to:
The principles that should be observed by all professionals working with children and young people who have SEN include:
All children and young people should expect to receive an education that enables them to achieve the best possible educational and other outcomes, and become confident, able to communicate their own views and ready to make a successful transition into adulthood, whether into employment, further or higher education or training.
Underpinning this should be a range of ‘best practice’ duties on schools:
All schools should have a clear approach to identifying and responding to SEN. The benefits of early identification are widely recognised – identifying need at the earliest point and then making effective provision improves long-term outcomes for the child or young person.
A pupil has SEN where their learning disability or disabilities calls for special educational provision, namely provision different from or additional to that normally available to pupils of the same age. Making higher quality teaching normally available to the whole class is likely to mean that fewer pupils will require such support. Such improvements in whole-class provision tend to be more cost effective and sustainable.
SEN support should be a graduated approach to supporting pupils with SEN.
Schools should assess each pupil’s current skills and levels of attainment on entry, building on information from previous settings and attainment where appropriate.
Class and subject teachers, supported by the senior leadership team, should make regular assessments of progress for all pupils. These should seek to identify pupils making less than expected progress given their age and individual circumstances. This can be characterised by progress which:
It can include progress in areas other than attainment – for instance where a pupil needs to make additional progress with wider development or social needs in order to make a successful transition to adult life.
Where a pupil is making less progress than expected, the first response to such progress should be high quality teaching targeted at their areas of weakness. Where progress continues to be less than expected the class or subject teacher, working with the responsible teacher for SEN, should assess whether the child has SEN. While informally gathering evidence (including the views of the pupil and their parents) schools should not delay in putting in extra teaching or other rigorous interventions designed to secure better progress, where required. The pupil’s response to such support can help identify their particular needs.
For some children, SEN can be identified at an early age. However, for other children and young people difficulties become evident only as they develop. All those who work with children and young people should be alert to emerging difficulties and respond early. In particular, parents know their children best and it is important that all professionals listen and understand when parents express concerns about their child’s development. They should also listen to and address any concerns raised by children and young people themselves.
Persistent disruptive or withdrawn behaviours do not necessarily mean that a child or young person has SEN. Where there are concerns, there should be an assessment to determine whether there are any causal factors such as undiagnosed learning disabilities, difficulties with communication or mental health issues. If it is thought housing, family or other domestic circumstances may be contributing to the presenting behaviour a multi-agency approach may be appropriate. In all cases, early identification and intervention can significantly reduce the use of more costly intervention at a later stage.
Professionals should also be alert to other events that can lead to learning disabilities or wider mental health difficulties, such as bullying or bereavement. Such events will not always lead to children having SEN but it can have an impact on well-being and sometimes this can be severe. Schools should ensure they make appropriate provision for a child’s short-term needs in order to prevent problems escalating. Where there are long-lasting difficulties schools should consider whether the child might have SEN.
Slow progress and low attainment do not necessarily mean that a child has SEN and should not automatically lead to a pupil being recorded as having SEN. However, they may be an indicator of a range of learning disabilities. Equally, it should not be assumed that attainment in line with chronological age means that there is no learning disability. For example, some children and young people may be high achieving academically, but may require additional support in communicating and interacting socially. Some learning disabilities occur across the range of cognitive ability and, left unaddressed may lead to frustration, which may manifest itself as disaffection, emotional or behavioural difficulties.
When reviewing and managing special educational provision there are four broad areas of need and support which give an overview of the range of needs that should be planned for, and schools should review how well equipped they are to provide support across these areas. They are:
Where a pupil is identified as having SEN, schools should take action to remove barriers to learning and put effective special educational provision in place. This SEN support should take the form of a four-part cycle (assess, plan, do, review) through which earlier decisions and actions are revisited, refined and revised with a growing understanding of the pupil’s needs and of what supports the pupil in making good progress and securing good outcomes. This is known as the graduated approach. It draws on more detailed approaches, more frequent review and more specialist expertise in successive cycles in order to match interventions to the SEN of children and young people.
Parents should be fully aware of the planned support and interventions and, where appropriate, plans should seek parental involvement to reinforce or contribute to progress at home. Parents should also be involved in reviews of support provided to their child and have clear information about the impact of the support and interventions, enabling them to be involved in planning next steps
Clear analysis is made of needs based on:
Following assessment, the teacher, specialist, parent/carers and pupil, agree on a plan of action to include:
All planning must be pupil centred and outcomes focussed and recorded.
All the pupil’s teachers and support staff are made aware of the plan and implement the adjustments, support and interventions. Teachers are responsible for:
The specialist supports teachers in the effective implementation of provision
Review – the quality, effectiveness and impact of provision is evaluated by the review date. This includes sharing information with pupil and parent/carers and seeking their views. The cycle then starts again at assess with the updated needs of the pupil being considered before planning a continuation of or change to provision.
Staged intervention is based on:
At STAGE 1 when a concern is identified (A parent, teacher, early years worker or anyone involved with the child may draw attention to this.):
At STAGE 2 when concerns/difficulties are ongoing:
At STAGE 3 if difficulties are severe, more complex and persistent:
SEN support should include planning and preparation for the transitions between phases of education and preparation for adult life. To support transition, the school should share information with the school, college or other setting the child or young person is moving to. Schools should agree with parents and pupils the information to be shared as part of this planning process.
Persons identified as having Sp.L.D. all show different intellectual and emotional profiles, strengths and weaknesses, learning styles and life experiences. Within this context, Sp.L.D. can be identified as distinctive patterns of difficulties, relating to the processing of information, within a continuum from very mild to severe, which may result in restrictions in literacy, language, number, motor function, short term memory and organisational skills.
In practice, the ‘experience’ of Sp.L.D. and/or experiences which causes individuals to become ‘delicate’ and vulnerable within an educational setting often leads to a rapid downward spiral in self-esteem/self-concept. Therefore, it is crucial to recognise the additional interrelated emotional and social needs of such ‘delicate‘ and vulnerable individuals. As such, a high priority should be given to providing a learning environment that caters for the diversity of emotional and learning needs in order to help these individuals achieve their potential.
Persons with Sp.L.D. have average or above average cognitive abilities (i.e. 90 or above measured IQ). In addition, as a result of unidentified Sp.L.D. there may be associated emotional and social difficulties, including behavioural issues.
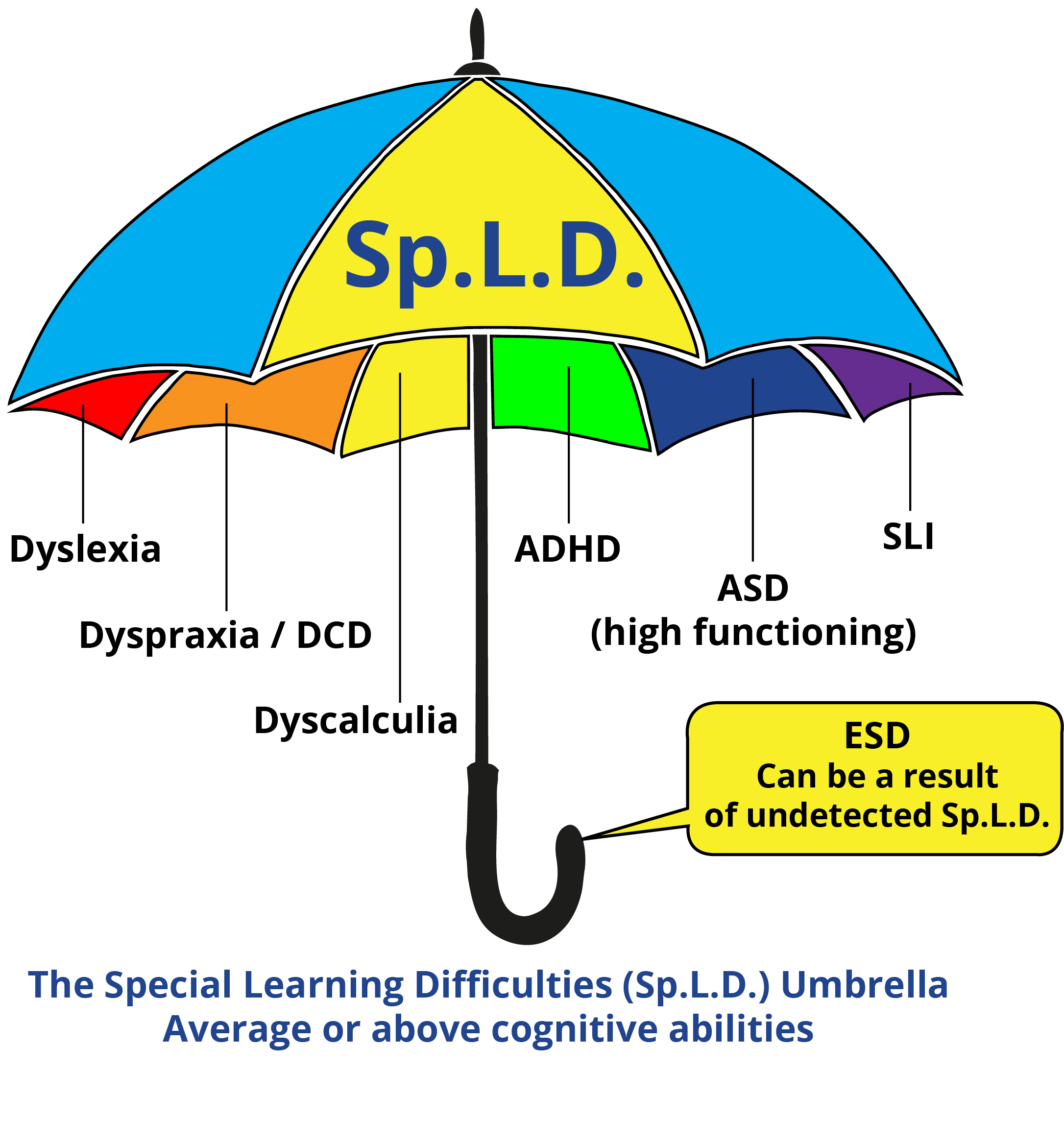
The definitions of each of the Sp.L.D. are at Annex A.
Central to many Sp.L.D. is the role of cerebellar functioning and also the inhibition of primitive reflexes. This, along with cognitive, behavioural and environmental factors can lead to the co-morbidity (overlap or co-existence) between indicators of Sp.L.D. and is the reason why many labels may be attached to the same students. When this occurs (whatever the etiology) the label which best describes these students is the umbrella term Sp.L.D. Children with co-existing Sp.L.D. experience even more difficulties within the learning situation. With the exception of the various educational/social approaches used to prepare the high-functioning ASD child for change (eg. visual timetable, story board), the pedagogical approaches, including social integration and independence skills, remain the same for all Sp.L.D. children including high-function ASD.
‘…in developmental disorders co-morbidity is the rule, not the exception.’
Kaplan and her colleagues (2001)
Correlation of co-morbidity of various Sp.L.D., including high-functioning ASD has been prevalent from the 1960’s. However, for a variety of reasons, few professionals have either understood its relevance or have been willing to make the ‘jump’ from research to practice. Fortunately, Ginny Russell and Zsuzsa Pavelka, have brought together much of the relevant research in their article ‘Children Who Share Symptoms of Autism, Dyslexia and Attention Deficit Hyperactivity Disorder’ (2013).
EU-28 POPULATION STATISTICS (Referring to the EU-28 Population Data)
Taken from eurosat – education and training in the EU, 8 February 2017:
References:
It is very difficult to establish the actual prevelance of Sp.L.D. in the EU-28 for two main reasons:
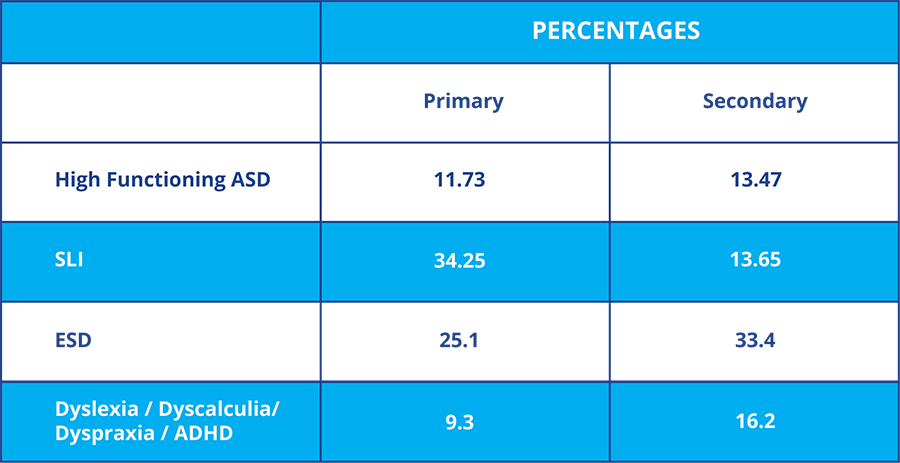
With the pro-rated percentage for High-functioning ASD, these are the actual Sp.L.D. statistics for England up to January 2014.
Therefore, taking a very conservative extrapolation of just half of all the above percentages for SLI and ESD, and using the above eurostat statistics [28 million enrolled in primary and 41 million in secondary education there could be an Sp.L.D. prevelance in the EU-28 of:
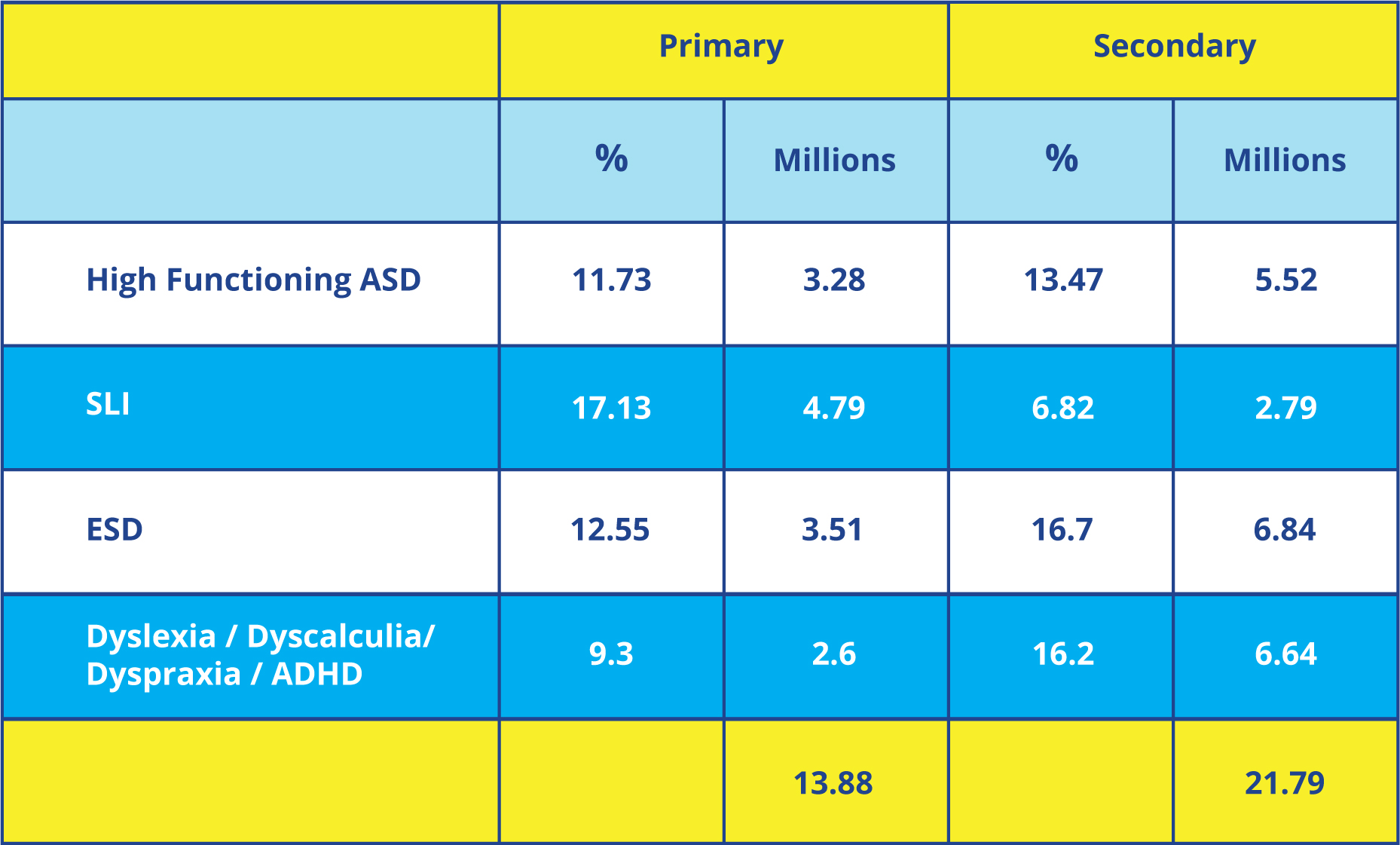
Between 13.88 millions in primary education and 21.79 millions in secondary education will have Sp.L.D. or a total of 35.67 million. Of course, this will exclude all persons with Sp.L.D. who have exited full-time education pre-2015 or who have Sp.L.D. in pre-primary or Tertiary Education. Moreover, this also excludes all the EU-28 adult population who have Sp.L.D.
Important factors:
In the worst case it can lead to criminal acts and imprisonment. In the school setting, a lack of professional knowledge of Sp.L.D. often leads to children being incorrectly labelled as ‘lazy, stupid or violent’. The reverse is also true where children and young persons, having had on-going support for their Sp.L.D., go on to higher education and become valuable citizens and employees or entrepreneurs. Early identification and intervention is therefore vital.
As shown above, there could have been 35.67 million persons with generally unidentified and unsupported Sp.L.D. in the EU-28 primary and secondary educations systems. For such a number to remain unidentified and, as a consequence unsupported, would be a massive lost generation that the EU cannot afford to lose in today’s global market. More importantly, the potential to translate lost generations into effective citizens will increase the GDP of all the EU-28 nations.
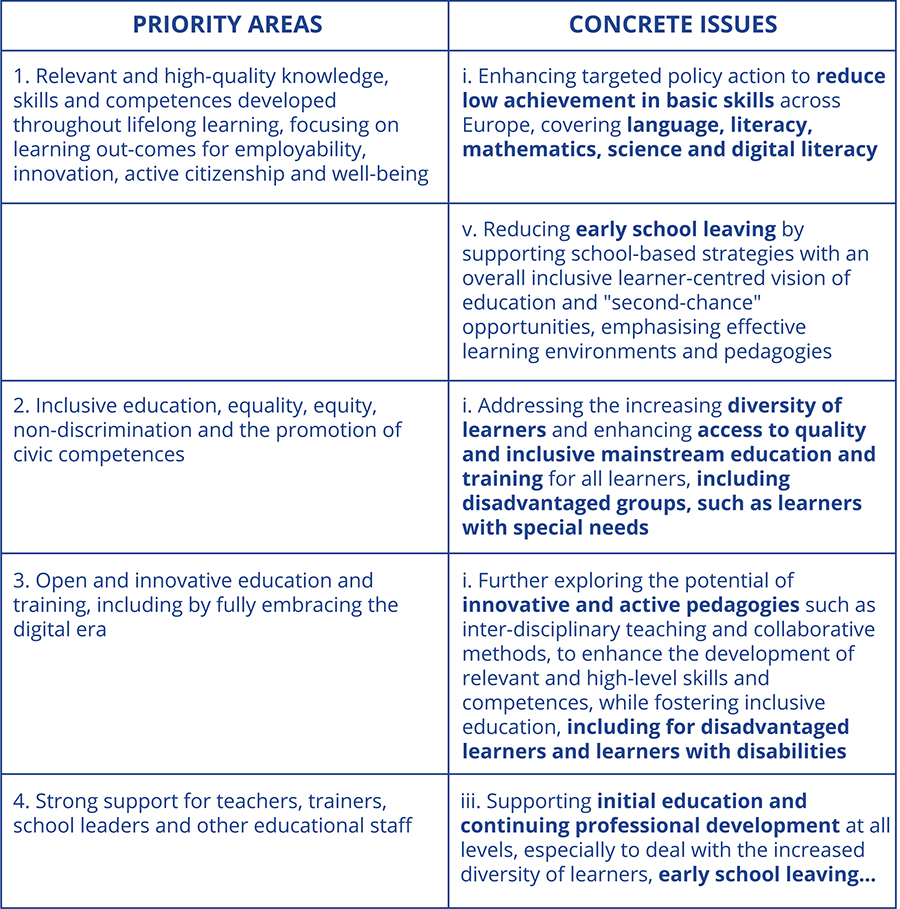
The following extracts from the ET2020 – Working Group Mandates 2016 -2018 highlight the relevance of this policy to the work of these Working Groups.
Suggested topics for peer learning activities, which WG members may modify or suggest additions to, include:
(4) Continuity across education levels: approaches (pedagogical, professional, structural) to: a) enhance continuity in education systems, from ECEC to primary and secondary levels; b) act as prevention mechanisms; and c) ensure the progression of skills and overall development of each child, including innovative forms of support for pupils with special needs (Priority Area 1).
Working Group on Promoting Citizenship and the Common Values of Freedom, Tolerance and Non-Discrimination through Education
The Paris Declaration adopted by Education Ministers on 17 March 2015 . The Declaration urges EU level actions “to cooperate and coordinate, to exchange experiences and to ensure that the best ideas and practices can be shared throughout the European Union” with a view to:
(3) Fostering the education of disadvantaged children and young people, by ensuring that our education and training systems address their needs;
The working group will also contribute to other ‘concrete issues’:
http://ec.europa.eu/social/main.jsp?catId=1137&langId=en
The following priority areas of the European Disability Strategy 2010-2020 are relevant:
The Erasmus Plus Project (2014-1-UK01-KA200-001652) which concludes in August 2017 has created an innovative world’s first ‘one-stop-shop’ for Sp.L.D Adult and Teacher Training in the English language. The Project has:
CONCLUSIONS
In 2015, there could have been 35.67 million persons with generally unidentified and unsupported Sp.L.D. in the EU-28 primary and secondary educations systems. This will exclude all persons with Sp.L.D. who have exited full-time education pre-2015 or who have Sp.L.D. in pre-primary or Tertiary Education. Moreover, this also excludes all the EU-28 adult population who have Sp.L.D.
For such a number to remain unidentified and, as a consequence unsupported, would be a massive lost generation that the EU cannot afford to lose in today’s global market. More importantly, the potential to translate lost generations into effective citizens will increase the GDP of all the EU-28 nations.
ET2020 is clear in its mandated priorities to:
The above stated Erasmus Plus Project meets priorities 1i; 1v; 2i; 3i and 4iii. Therefore, it is clear that the Project website should be urgently translated to provide unhindered access to the Sp.L.D. information for our EU citizens and teachers.
Mr. Colin Lannen & Dr. Sionah Lannen
Project Co-ordinators
Erasmus + Project: 2014-1-UK01-KA200-001652
12 February 2017
Persons with Sp.L.D. have average or above average cognitive abilities (i.e. 90 or above measured IQ). In addition, as a result of unidentified Sp.L.D. there may be associated emotional and social difficulties, including behavioural issues.
Persons identified as having Sp.L.D. all show different intellectual and emotional profiles, strengths and weaknesses, learning styles and life experiences. Within this context, Sp.L.D. can be identified as distinctive patterns of difficulties, relating to the processing of information, within a continuum from very mild to severe, which may result in restrictions in literacy, language, number, motor function, short term memory and organisational skills.
In practice, the ‘experience’ Sp.L.D. and/or experiences which causes individuals to become ‘delicate’ and vulnerable within an educational setting often leads to a rapid downward spiral in self-esteem/self-concept. Therefore, it is crucial to recognise the additional interrelated emotional and social needs of such ‘delicate‘ and vulnerable individuals. As such, a high priority should be given to providing a learning environment that caters for the diversity of emotional and learning needs in order to help these individuals achieve their potential.
The common neurodevelopmental disorders (disabilities/difficulties) include dyslexia, ADHD, dyspraxia, SLI, and dyscalculia. There is considerable symptom overlap in particular between ADHD and dyslexia, and like autism both are described as developmental disorders by psychiatric classification systems. Overlapping conditions are termed co-morbidity and these may reflect the greater difficulties experienced by children with a combination of deficits. Sometimes it is apparent that many children with a developmental disorder could be classified in several ways.
Although there are numerous definitions of the Sp.L.D. the definitions and explanations that should be used are based on decades of practical work with both children, young people and adults with Sp.L.D.
Both Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM V) and the International Classification of Diseases (ICD-10) have various definitions and diagnosis criterion for Sp.L.D. However, although useful to dip in and out of for the purposes of personal study and comparison, the definitions and explanations used in this document are more widely understood and recognised in the field of Special Educational Needs, particularly by teachers and parents.
Dyslexia is a learning difficulty that primarily affects the skills involved in accurate and fluent word reading and spelling. Dyslexia is defined as a learning difficulty that affects reading and spelling abilities. Dyslexia has historically been understood as the unexpected difficulties some otherwise intelligent pupils have when learning to read and spell.
The core features of dyslexia are difficulties with:
Difficulties in these areas can be thought of as reflecting a core weakness in the systems that are involved in processing information about word-sounds (phonology) and their impact is primarily seen on the development of decoding and encoding skills in reading and spelling.
In addition to these characteristics, it is acknowledged that the visual and auditory processing difficulties that some individuals with dyslexia can experience, and points out that dyslexic readers can show a combination of abilities and difficulties that affect the learning process. Some also have strengths in other areas, such as design, problem solving, creative skills, interactive skills and oral skills.
Co-occurring difficulties may be seen in aspects of language, motor co-ordination, mental calculation, concentration and personal organisation, but these are not, by themselves, markers of dyslexia.
Some other defintions of Dyslexia include:
EDA Definition
Dyslexia is a difference in acquiring reading, spelling and writing skills, that is neurological in origin.
The cognitive difficulties that cause these differences can also affect organisational skills, calculation abilities etc. It may be caused by a combination of difficulties in phonological processing, working memory, rapid naming, sequencing and the automaticity of basic skills. Alongside these issues is the ongoing challenge for people with dyslexia navigating through life in a largely non-dyslexia friendly world.
Researchers acknowledge that there are many possible causes of dyslexia, including genetics.
There is no relationship between a person’s level of intelligence, individual effort of socio-economic position and the presence of dyslexia.
Furthermore, across Europe the diversity of languages and the multilingual demands, socio-cultural backgrounds as well as educational opportunity, have a significant influence on the life-chances for dyslexic children and adults.
In addition to these characteristics, it is acknowledged that the visual and auditory processing difficulties that some individuals with dyslexia can experience, and points out that dyslexic readers can show a combination of abilities and difficulties that affect the learning process. Some also have strengths in other areas, such as design, problem solving, creative skills, interactive skills and oral skills. (British Dyslexia Association)
Dyslexia is a specific learning difficulty that mainly affects the development of literacy and language related skills. It is likely to be present at birth and to be life-long in its effects. It is characterised by difficulties with phonological processing, rapid naming, working memory, processing speed, and the automatic development of skills that may not match up to an individual’s other cognitive abilities.
It tends to be resistant to conventional teaching methods, but its effect can be mitigated by appropriately specific intervention, including the application of information technology and supportive counseling.
What is it?
Dyspraxia [also known as Developmental Coordination Disorder (DCD)] can affect any or all areas of development – intellectual, emotional, physical, language, social and sensory – and may impair a person’s normal process of learning. Usually, it’s said to be an impairment or immaturity of the organisation of movement. However, associated with this may be problems of language, perception and thought.
Problems arise in the process of forming ideas, motor planning and execution, since those with dyspraxia have poor understanding of the messages their senses convey and difficulty relating those messages to actions. This means physical activities are hard to learn, difficult to retain, and hesitant and awkward in performance.
Signs and Symptoms
Other defintions of Dyspraxia:
EU Commission Scientific Committees
Dyspraxia is a disability that affects body movements and co-ordination. It often leads to clumsiness, and problems with language, perception and thoughts. The causes are unclear, but it can be acquired via a stroke, accident, illness, weak trauma, momentary lack of oxygen at birth or during pregnancy. The condition can be treated via early intervention, using physical and occupational therapy to improve motor skills.
European Academy of Childhood Disability
They use the DSM V and the ICD-10 definitions.
Dyspraxia, a form of developmental coordination disorder (DCD) is a common disorder affecting fine and/or gross motor coordination in children and adults. It may also affect speech. DCD is a lifelong condition, formally recognised by international organisations including the World Health Organisation. DCD is distinct from other motor disorders such as cerebral palsy and stroke, and occurs across the range of intellectual abilities. Individuals may vary in how their difficulties present: these may change over time depending on environmental demands and life experiences.
An individual’s coordination difficulties may affect participation and functioning of everyday life skills in education, work and employment.
Children may present with difficulties with self-care, writing, typing, riding a bike and play as well as other educational and recreational activities. In adulthood many of these difficulties will continue, as well as learning new skills at home, in education and work, such as driving a car and DIY.
There may be a range of co-occurring difficulties which can also have serious negative impacts on daily life. These include social and emotional difficulties as well as problems with time management, planning and personal organisation, and these may also affect an adult’s education or employment experiences.
Many people with DCD also experience difficulties with memory, perception and processing. While DCD is often regarded as an umbrella term to cover motor coordination difficulties, dyspraxia refers to those people who have additional problems planning, organising and carrying out movements in the right order in everyday situations. Dyspraxia can also affect articulation and speech, perception and thought.
The information processing problems which cause students to experience difficulties of a dyslexic nature e.g. short term memory, the sequencing and organisation of information and the speed of information processing can also cause difficulties in many areas of mathematics. The term often given to describe this is dyscalculia.
The nature of the difficulties which are experienced by students with dyscalculia include the following:
Mathematics also has its own language and this can be at the root of many problems. General mathematical terminology with words like perimeter,value and equals may be unfamiliar. It is interesting to ask a class to define the word ‘equals’ and discover the many different replies, perhaps most commonly that it means ‘answer’. These words all need to be clearly understood before they can be used in calculations.
To complicate matters further, one single mathematical process can be described with a wide variety of terms. For instance, multiply,times, product,of or add, increase, plus, sum and total.
Mathematics has an interrelating/sequential structure. It is a subject in which one learns the parts. The parts build on each other to make a whole. Knowing the whole enables one to reflect with more understanding on the parts, which in turn strengthens knowledge of the whole. Knowing the whole also enables one to understand the sequences and interactions of the parts and the way they support each other.
Since the central problem is likely to be that of relating symbols to the operations which they represent, it makes good sense for the student to first carry out the operations using structured materials. Then they should be shown how to describe symbolically what they have been doing.
Students with dyscalculia are better at ‘doing’ than at ‘naming’ and a foundation of ‘doing’ is essential.
The great advantage of using structured materials is that they ensure that ‘doing’ comes first and ‘naming’ afterwards. If the order is reversed, one is essentially confronting the student with dyscalculia with a mass of bewildering symbols and technical terms while not letting him/her have any clear idea of what he/she is supposed to do with them. Once the necessary foundations have been acquired by ‘doing’, however, abstract reasoning, generalisations and discoveries should then follow.
Concrete materials which are recommended for students with dyscalculia at the primary and high school level include Cuisenaire Rods, Dienes Multilbase Arithmetic Blocks and Montessori material etc. Students with dyscalculia may have to rely on concrete materials for a longer period of time than their peers since they often find it difficult to memorise number bonds.
When teaching Mathematics to students with dyscalculia therefore, the principles of multisensory teaching (visual, auditory, tactile-kinaesthetic) which apply to language work should also apply mathematics. For example, new mathematical concepts and processes should be introduced using concrete materials, diagrams, pictures and verbal explanation. Then the student should be asked to explain the process, instructions etc. in his/her own words. Progress should be carefully monitored at each stage, checking that a particular concept has been thoroughly mastered and understood before moving on to the next step.
What is it?
All individuals with Sp.L.D. have short-term memory difficulties. This manifests itself, among other things, in concentration difficulties. When these concentration difficulties become so severe as to interfere with the child’s ability to cope within all settings it is usually referred to as ADHD.
A variety of so called solutions are ‘out there’ from medication with stimulant drugs, diet and alternative ‘drug free’ therapies. None offer a complete solution but in combination with behavioural programmes may reduce the symptoms and, in particular, those ‘challenging’ behaviours.
Other definitions of ADHD:
ADHD-Europe
http://www.adhdeurope.eu/links/68-sites-on-adhd.html
Attention-Deficit/Hyperactivity Disorder (AD/HD) is defined as a developmentally inappropriate level of inattention and/or hyperactivity-impulsivity that is present before the age of seven years.
AD/HD is:
Ideally, early and accurate detection in conjunction with appropriate treatment of AD/HD, support for the family and interventions/accommodations within the educational and professional systems are critical for an individual. The hyperactive or impulsive behaviours and attention deficit problems are often not in keeping with either the intellectual abilities or the developmental stages of the individual. (European Interdisciplinary Network for AD/HD Quality assurance [EINAQ], 2004)
http://www.adhd-institute.com/disease-management/guidelines/european-guidelines/
The most recent European clinical guidelines for ADHD were published by the European Society for Child and Adolescent Psychiatry (ESCAP) in 2004. European guidelines for the use of long-acting medication in patients with ADHD were also published in 2006. Another widely consulted source of guidance for clinicians working in ADHD is the 2009 update of the UK National Institute for Health and Clinical Excellence guidelines which provide comprehensive recommendations for the diagnosis and management of ADHD. European guidelines also recognise the importance of adequately managing the important transition period between adolescent and adult services, and these are addressed specifically in both the NICE clinical guidelines and in guidance from the British Association of Pharmacology.
Diagnosis based on presence of clear evidence of clinically significant impairment in social, academic or occupational functioning. Impairment implies a higher severity or frequency of symptoms, in addition to interference with functioning in major life domains:
Attention deficit hyperactivity disorder (ADHD) is one of the most common childhood disorders and it can continue through adolescence and into adulthood. Symptoms include difficulty staying focused and paying attention, difficulty controlling behaviour, and hyperactivity (over-activity).
ADHD has three subtypes:
Predominantly inattentive. The majority of symptoms (six or more) are in the inattention category and fewer than six symptoms of hyperactivity-impulsivity are present, although hyperactivity-impulsivity may still be present to some degree.
Children with this subtype are less likely to act out or have difficulties getting along with other children. They may sit quietly, but they are not paying attention to what they are doing. Therefore, the child may be overlooked, and parents and teachers may not notice that he or she has ADHD.
Combined hyperactive-impulsive and inattentive. Six or more symptoms of inattention and six or more symptoms of hyperactivity-impulsivity are present.
Most children have the combined type of ADHD.
What is it?
SLI is a form of language impairment that is diagnosed when language abilities are below age expectations but non-linguistic developmental abilities are within age expectations. A child’s first words are likely to be delayed, early grammatical forms may be late to appear, vocabulary size can be smaller and less varied than expected, awareness of the phonemic and spelling structure of words can be delayed well into the school-age years, and utterances can be shorter and less complex than expected. Language performance will be below age expectations as measured by an individualized, standardized, culturally and linguistically appropriate psychometric measure. Nonverbal intellectual performance is not impaired.
The low language abilities result in functional limitations in effective communication, social participation, academic achievement, or occupational performance, alone or in any combination.
Symptoms will be present in early childhood (but may not become fully manifest until language demands exceed limited capacities).
Dyslexia and SLI were for many years treated as distinct disorders but are now often regarded as different manifestations of the same underlying problem, differing only in severity or developmental stage. The merging of these categories has been motivated by the re-conceptualisation of dyslexia as a language disorder in which phonological processing is deficient.
Many individuals who have a history of mild language difficulties (in grammar and vocabulary for example) often not severe enough to need speech and language therapy go on to have literacy difficulties. Individuals with SLI often also have literacy difficulties. Dyslexia is often described by researchers as a difficulty which is based in language. Early difficulties with speech sound production, for instance children whose speech is difficult to understand, are thought to affect literacy skills only when the difficulties remain past the sixth birthday. Even then some pupils with these difficulties hear and understand speech sounds well despite their speech difficulties and so experience no particular phonologically based difficulties with literacy.
One of the characteristics of dyslexia is slow access to verbal labels. This is typically measured by asking children to name sequences of pictures or digits but sometimes also just by picture or object naming. If there are significant difficulties in gaining rapid access to the names of things this can affect everyday communication; words do not come to mind easily.
Difficulties retaining spoken information in short term and working memory is another of the characteristics of dyslexia and this too can affect both comprehension and expression. Short term and working memory are needed for the temporary storage of incoming information and processing information or ‘making sense out of it’. Reduced efficiency of working memory can contribute to comprehension problems, especially when information is given in a complex or confusing way. Similarly working memory is needed to help store and organise words for spoken expression so inefficiencies in this area can contribute to expressive language difficulties.
Research has found that those individuals with dyslexia who have good vocabulary and grammar skills alongside their difficulties with phonology are to some extent protected from the poorest outcomes in literacy development. This is thought to be because they can use their language skills to support their poor phonological skills. For instance they may use the context of a passage to work out an unknown word, boosting their unreliable phonic decoding. These individuals typically find reading single words out of context more difficult than reading a passage.
http://www.afasic.org.uk/professionals/sli/
Some children do not develop speech and language as expected. They may experience difficulties with any or all aspects of speech and language – from moving the muscles which control speech to the ability to understand or use language at all. These difficulties can range from the mild to the severe and long-term.
Sometimes these difficulties are unrelated to any other difficulty or disorder – they are therefore said to be specific language difficulties. Some children may have both a specific language difficulty and other disabilities.
Education and participation in society depend upon the ability to communicate. It is vital that children with speech and language impairments are offered comprehensive help as early as possible.
Within these areas some children may have difficulties in understanding language (receptive difficulties), some in using language (expressive difficulties), and some in both understanding and using language.
http://www.cplol.eu/eng/SLT.html
The speech and language therapist / logopedist is concerned with communication and with language, and treats all disorders of speech, voice and spoken and written language, regardless of aetiology, in children, adolescents, adults and the elderly. The speech and language therapist is the professional responsible for the prevention, assessment, treatment and scientific study of human communication and associated disorders. In this context, communication encompasses all those processes associated with the comprehension and production of spoken and written language, as well as appropriate forms of non-verbal communication.
The distinction has been made between ASD and high-functioning ASD where the individuals are not cognitively challenged, have average or above average intellectual abilities and can speak, read, and write. Often individuals with high-functioning ASD have co-morbidity of other Sp.L.D.
The triad of impairments are three areas of difficulty which all people with ASD share. They vary from one person to another but they seem to be common.
Persons with ASD experience difficulties in social interaction and communication and have rigid and repetitive ways of thinking and behaving. These behaviours are thought to be underpinned by difficulties in both the flexible generation of ideas and the understanding of other people’s thoughts and feelings. Sensory difficulties are common. These include being either over or under-sensitive to particular sensations or developing a particular interest in them.
There is great variation in the way that individuals with ASD show these different behaviours. Between 35 to 50 % of individuals with ASD have an additional learning disability, whereas others have average or advanced intellectual abilities. Difficulties with understanding and expressing language vary enormously. For some individuals spoken language is limited or absent altogether, while for others speech can be fluent but their use of language to communicate can often lack the conventional social content and timing, e.g. conversational turn taking.
Furthermore, stereotyped and inflexible behaviours range from repetitive movements of the body to idiosyncratic special interests, e.g. prime numbers, train timetables, and an insistence on sameness.
ASD is therefore a developmental condition and the presentation in any individual will change with age, with some experiencing periods of rapid improvement and others static or plateauing of development.
All schools are likely to include pupils who lie somewhere on the autism spectrum. The prevalence of ASD is believed to be at least four times higher in boys than girls, but the reasons for this gender difference have not yet been determined. ASD has a strong genetic component, although it is now recognised that this consists of both heritable and sporadic (non-inherited) forms. Non-genetic factors may also play a role in causing ASD, but such instances – often relating to environmental factors – probably account fewer cases and have yet to be identified.
Until recently, many children with autism were not diagnosed until four or five years of age, and even later for those with good language skills and of average or above average ability (‘high functioning autism’). However, progress has been made in the earlier identification of autism, and many children, especially those with a more classic presentation of autism in combination with language and motor skills delay, are now often identified before the age of five years.
When selecting therapies/ intervention for ASD the following factors need to be considered:
A theoretical understanding of ASD provides a useful framework for appreciating some of the potential differences between a person on the autism spectrum and a more typically developing person.
Many people are guided in their interaction with the social world by what may be called a social ‘instinct’, however, an individual with autism may not have this social instinct and may, instead, have to approach social situations cognitively or intellectually. This means that they may need to think through the expected social conventions in any situation, rather than instinctively understand what is required or how to behave. This is requires more effort and so social encounters can be very tiring and stressful as pupils have, literally, to work things out theoretically. Temple Grandin, a very able adult with high-functioning ASD, has said that ‘continually trying to work out what to do and what to say is like doing quadratic equations in your head.’
Another able adult with high-functioning ASD, Jim Sinclair, explains how he views autism.
‘Being autistic does not mean being inhuman. But it does mean being alien. It means that what is normal for other people is not normal for me, and what is normal for me is not normal for other people. In some ways I am terribly ill-equipped to survive in this world, like an extra-terrestrial stranded without an orientation manual.
But my personhood is intact. My selfhood is undamaged. I find great value and meaning in my life and I have no wish to be cured of being myself. If you would help me, don’t try to change me to fit your world. Don’t try to confine me to some tiny part of the world that you can change to fit me. Grant me the dignity of meeting me on my own terms, recognise that we are equally alien to each other, that my ways of being are not merely damaged versions of yours. Question your assumptions. Define your terms. Work with me to build more bridges between us.’
The implications of finding the social world confusing, impenetrable or alienating are significant, for example:
We anticipate what will happen in an interaction by our social ability to predict what is expected and likely to occur. Temple Grandin, tells us:
‘Social interactions that come naturally to most people can be daunting for people with autism. As a child, I was like an animal that had no instincts to guide me; I just had to learn by trial and error. I was always observing, trying to work out the best way to behave, but I never fitted in…I wanted to participate, but did not know how.’
We are helped in our predications by our capacity to read the interactional ‘subtext’, not only what the person is saying to us, but what they mean by what they are saying, what the unspoken messages are. One 18-year-old young man with autism as saying: ‘People send each other messages with their eyes and I don’t understand those messages.’
We are informed by social conventions that guide us in our relating ‘styles’; for example, the conventions of the classroom, e.g. putting up a hand to answer or ask a question may also apply in situations, such as school assembly but may not in other school settings, such as talking with friends at the lunch table.
Shared social conventions help us to focus on shared, relevant aspects of the social environment. Generally, for example, we understand that we need to look at the person speaking to us, or to signal that we are listening even when we are unable to look. We are able to pick out the salient aspects of a situation and these provide us with helpful social information. There are also, for example, conventions about the extent to which we interact with people when we enter a room dependent on familiarity and context. People with autism may be drawn to the non-social aspects of the room. For example, a very able woman with autism says that:
‘Autism is the inability to single out people as special, separate, unique entities – different from bits of the furniture, different from even the family pet dog.’
The term used to describe how typically developing individuals use attention, i.e. with several interests are aroused at any given time is polytropism. Typical individuals are able to divide and shift attention and multi-task. Those on the autism spectrum however are more likely to be monotropic – much less able to divide and shift their attention and are likely to be very focused on a single activity or interest. A High-functioning ASD individual has said that when absorbed on a task, she often literally becomes ‘deaf’ to the requests of others and finds it hard to refocus quickly on a different task. In school, pupils are frequently called upon to multitask and to switch quickly from one topic or task to another, so pupils on the autism spectrum may be unable to keep track and are then often behind other pupils in organising their thoughts, belongings and actions.
Anxiety is a natural reaction to social situations that are unpredictable. A High-functioning ASD individual, has written much about his levels of anxiety which were so extreme that he experienced them as terror:
‘I have no idea how many ways there are to deal with a level of fear so great that is hangs over you like a storm cloud. The three remedies I chose and that made the most sense to me in all areas of my life were repetition, repetition and repetition.’
Delay or lack of development of speech without compensating gesture.
Some children with autism do not use spoken language to express themselves throughout their lives. Others may use a small number of spoken words to express basic needs. A minority do go on to use spoken language skilfully but often this can place considerable demands on the individual.
Sensory processing difficulties in the different domains:
Other definitions of High-functioning ASD:
http://www.neuron-eranet.eu/en/261.php
European High-functioning Autism network (EUHFAUTISM): Translational research in a phenotypically well characterised sample
Individuals with ESD cover the full range of ability and continuum of severity. Their associated behaviours present a barrier to learning and persist despite the implementation of an effective school behaviour policy and personal/social curriculum. They may be withdrawn or isolated, disruptive and disturbing, hyperactive and lack concentration, have immature social skills or present challenging behaviours.
ESD can manifest itself in a variety of ways: individuals can be physically or verbally aggressive; they can harm themselves or suffer from anxiety or depression; they can be withdrawn or uncommunicative. Individuals who are withdrawn or emotionally fragile are as much a part of the ESD continuum as those who act in more demonstrative ways. Many factors may underpin a individual’s ESD, including the painful impact of abuse or trauma, hitherto unidentified Sp.L.D.
In dealing with ESD – establishing positive relationships are key, including:
Key to any successful intervention and learning with individuals with ESD is their emotional, social and physical wellbeing. This should be positively developed by fostering a safe, caring, supportive, purposeful environment that enables the development of relationships based on mutual respect. The three aspects of wellbeing are inextricably linked.
The range of approaches to positive relationships and behaviour include:
Framework for Intervention/Staged Intervention (FFI/SI) is an approach to the management of low-level disruptive behaviour in the classroom. It uses a peer support model, enabling teachers to support each other in forming solutions. While the focus is on low-level disruption, there is considerable evidence that FFI/SI can prevent minor problems from escalating into major ones. The highest level of the framework offers a mechanism to track higher level problems if they do occur.
Restorative approaches offer a powerful approach to promoting harmonious relationships in schools and can lead to the successful resolution of conflict and harm.
Restorative approaches range from:
School ethos, policies and procedures need to be developed to support this work. The focus is on prevention and the involvement of the whole school community is paramount. It is a framework within which existing good practice can develop.
Key principles of restorative approaches:
Pupils seek fairness from adults who are dealing with disciplinary issues. Whether they are a perpetrator or a victim, their focus is not on winning or losing, but on trusting in a fair process. Restorative approaches help teachers ensure that pupils, staff and parents can be part of a fair process, while helping all involved to understand the impact of their behaviour on others.
Restorative approaches can:
Restorative approaches can be used at different levels in school:
Peer mediation is a process where those involved in a disagreement volunteer to discuss the issues and explore how best to take matters forward. It requires them to operate within a whole school ethos, which is itself restorative.
Children and young people can be more comfortable talking to someone their own age who understands their concerns and their perspective. Pupils learn to listen to others’ points of view and to accept differences.
In peer mediation pupils are trained to act as mediators in a dispute without help from teachers. This empowers children and develops their sense of community and co-operation. The school and classroom become more peaceful, allowing more teaching and learning to take place.
Peer mediation takes place in a structured and safe environment with adult supervision nearby and always requires the participation of two peer mediators. Peer mediators deal with low-level disputes and always refer to school staff when a situation becomes too complex for them to handle.
Peer mediation can provide a safe structure for children and young people to solve their problems and learn to negotiate.
Peer support can reinforce a positive ethos and sustain pupil motivation, just as peer rejection could turn schools into cold and inhospitable places.
Peer mediation can build a supportive environment and help to sustain the overall wellbeing within a school.
All pupils learn the basic skills of communication and conflict resolution and develop the coping skills that they will need outside and beyond school.
Pupils who are trained as peer mediators develop additional skills in communication, negotiation, understanding and problem solving. Acting as mediators helps to promote young people’s emotional and social skills and builds self-esteem and confidence.
It is essential that members of the school staff are trained with the pupils and operate to provide continuous support to the peer mediators.
A normal process of peer mediation training within a school might see a whole year group undergoing basic training in conflict handling and communication skills, followed by a selection process for peer mediators, which might include an open application and selection procedure.